

HIV Index Testing
Using a CQI Approach to Increase HIV Index Testing Services in Mwanza Region
The HIV index testing model involves the provision of HIV testing services (HTS) to sexual contacts and biological children less than 15 years of age of known HIV index clients. This model has demonstrated a significant increase in the identification of HIV positive cases among children and adults, and linkage-to-care and treatment services.
HIV index testing services were officially launched in Tanzania in 2019. By national targets, index sexual contact elicitation was set at 2:1, i.e., two sexual contacts per one HIV client. HIV index testing, being a new concept, was received with much skepticism at inception and faced many implementation challenges, especially on the elicitation of sexual contacts.
The Challenge
The Ciheb Tanzania–REACH project QI team, in collaboration with the Ariel Glasser Pediatric AIDS Healthcare Initiative (AGPAHI), the facility-level implementing partner, and the regional and council health management teams in Mwanza Region, conducted a retrospective facility-level HIV index testing performance review. The review, which was for performance between January and April 2019, revealed low uptake of index testing services in 16 high-volume facilities in Mwanza Region.
Index sexual partner elicitation remained consistently low at less than one sexual contact per one index client. Using a fishbone analysis, we identified the performance gap to be associated with: inadequate skills among healthcare providers on sexual contacts elicitation, fear of confidentiality among clients, lack of an effective way to reach elicited contacts at remote areas, documentation gaps due to inadequate space on improvised index testing register, lack of routine data use for performance monitoring, and inadequate collaboration between community and facility implementing partner to facilitate a continuum of care.
The graphs and the data table below show the index clients sexual contacts elicitation ratio trend from January to April 2019 in 16 high-volume facilities in Mwanza Region.
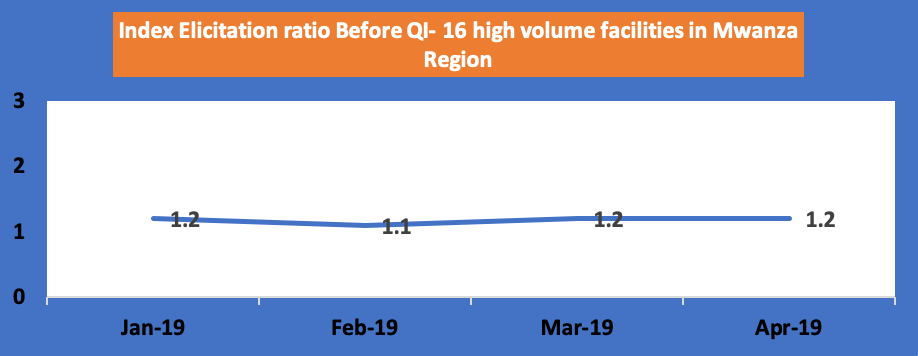
| Month | Jan-19 | Feb-19 | Mar-19 | Apr-19 |
|---|---|---|---|---|
| Index clients | 829 | 990 | 5,252 | 7,017 |
| Elicited contacts | 960 | 1095 | 6,516 | 8,374 |
| Elicitation ratio | 1.2 | 1.1 | 1.2 | 1.2 |
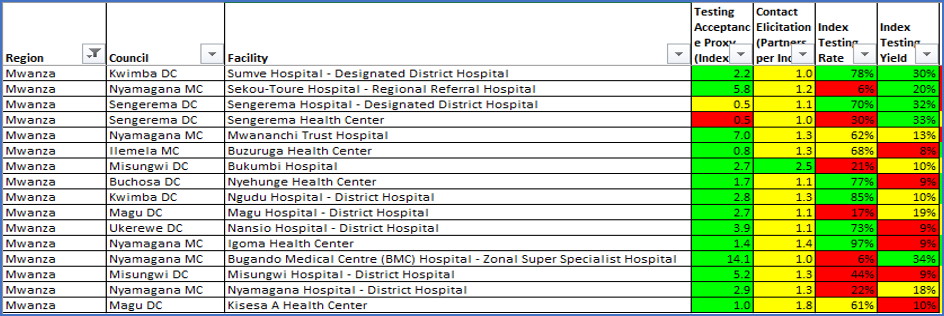
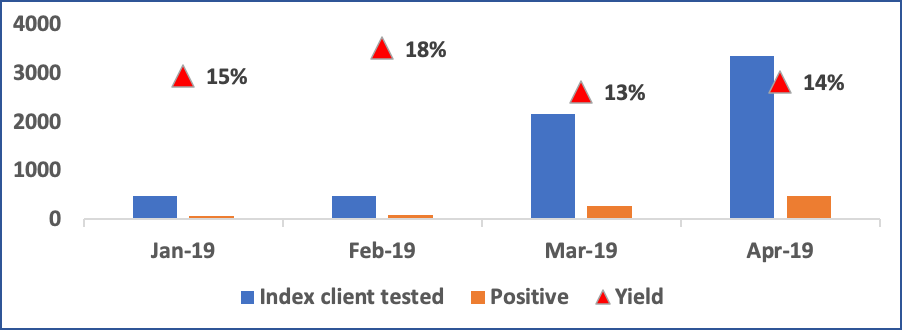
The chart below shows the performance on index testing services at 16 priority facilities in Mwanza Region as of April 2019 (before QI).
Index testing yield trend for 16 tier one facilities in Mwanza (before QI).
The Intervention
Ciheb directly supported quality improvement (QI) activities in these high-volume facilities. For HIV index testing, we aimed to improve two HIV index testing process indicators, 1) sexual contact elicitation ratio and 2) HIV index testing coverage. We also monitored HIV positivity yield from index testing services as compared to HIV positivity yield by other HIV testing modalities. We mainly focused on HIV index testing services among newly enrolled HIV positive clients and those with high viral load. We also supported facilities in ensuring all clients on antiretroviral treatment who missed the opportunity for HIV index testing services were provided with the services. In collaboration with regional and council health management teams and AGPAHI, we started implementing a QI initiative to improve HIV index testing services from May 2019.
AGPAHI organized the training of healthcare providers on index testing. We continued with on-site training and mentorship to healthcare practitioners to enhance their elicitation skills, partner notification services, patient confidentiality, and timely linkage of newly identified HIV-positive clients for index testing services. Ciheb also worked with ICAP, the community-level implementing partner, to support those conducting index testing by guiding them on how to reach out to elicited sexual contacts out of the facility for testing services.
Through such initiatives, we managed to build a culture for facilities to review their data for performance monitoring weekly. Working improvement teams at the facility level conducted monthly meetings to share experiences and each facility dedicated an Index focal person to continuously monitor the implementation of proposed tests of changes
The Results
Beginning May 2019, following the implementation of the tested changes mentioned above, we started seeing an improvement in the number of sexual contacts elicited per each HIV positive index client.
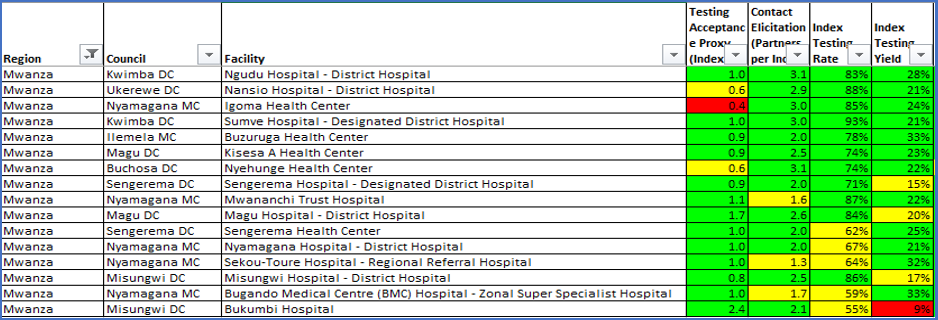
The charts below show significant improvement over time on the number of sexual partners elicited per each index client and the HIV positivity yield.
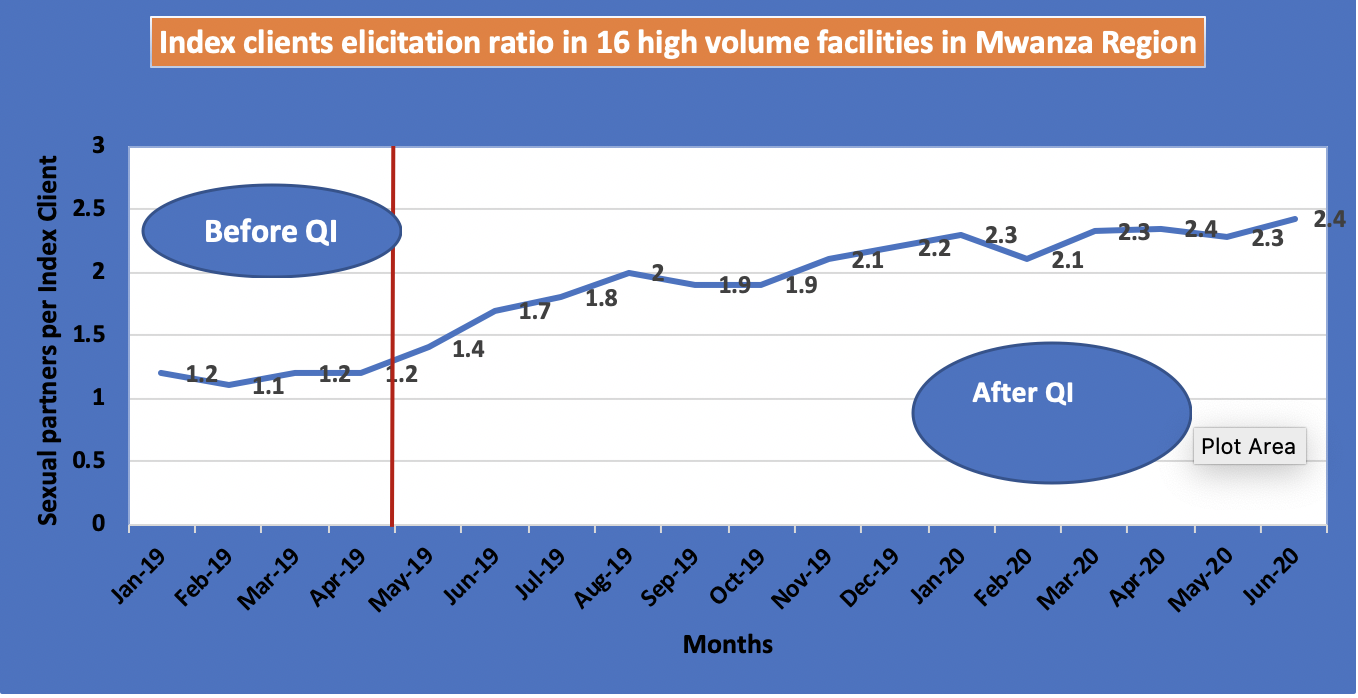
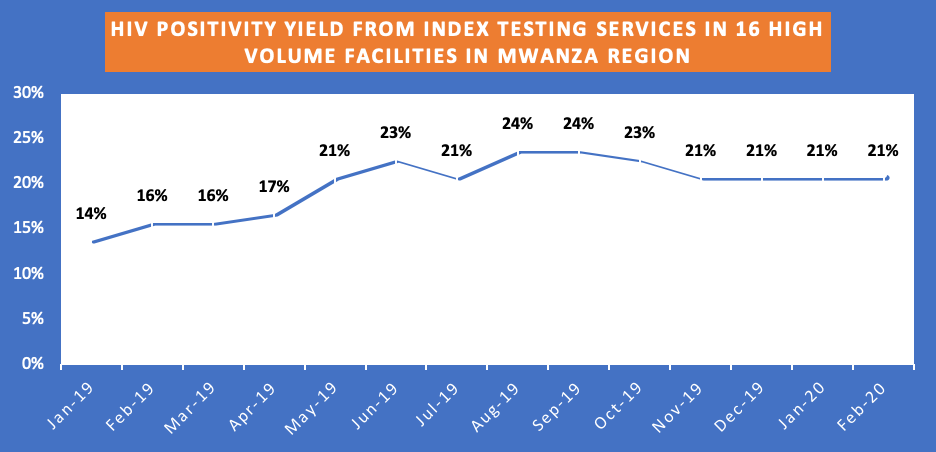
Monthly performance on index testing service at 16 priority facilities in Mwanza as of July 2020.
Lesson Learned
Through this CQI initiative, we have learned that enhancing provider skills is vital to ensure that index testing services are well implemented and monitored. Regular data use for performance review helps to identify gaps and promptly implement contextual solutions. Consistent and continuous technical assistance at all levels is paramount to address any knowledge gaps among new staff due to staff turnover or any programmatic updates. We also learned that the availability of a HIV index testing focal person in each facility is essential to coordinate services and ensure daily performance monitoring.
Challenges
Since the documentation of HIV index testing services is still paper-based, challenges on data accuracy remain. Also, some elicited contacts come from geographical regions that are outside the catchment areas of facilities, making tracing efforts extremely difficult. Ciheb has since developed an index contact tracer (ICT), a mobile-based application that helps in tracking contacts across all regions.
Story Written by Dr. Freddy Frank, Technical and Program Quality Advisor
Reviewed by Patience Komba, Associate Director Program Quality